




|
| |
|
| |
|
|
|
|
|
TCHS 4O 2000 [4o's nonsense] alvinny [2] - csq - edchong jenming - joseph - law meepok - mingqi - pea pengkian [2] - qwergopot - woof xinghao - zhengyu HCJC 01S60 [understated sixzero] andy - edwin - jack jiaqi - peter - rex serena SAF 21SA khenghui - jiaming - jinrui [2] ritchie - vicknesh - zhenhao Others Lwei [2] - shaowei - website links - Alien Loves Predator BloggerSG Cute Overload! Cyanide and Happiness Daily Bunny Hamleto Hattrick Magic: The Gathering The Onion The Order of the Stick Perry Bible Fellowship PvP Online Soccernet Sluggy Freelance The Students' Sketchpad Talk Rock Talking Cock.com Tom the Dancing Bug Wikipedia Wulffmorgenthaler |
|
bert's blog v1.21 Powered by glolg Programmed with Perl 5.6.1 on Apache/1.3.27 (Red Hat Linux) best viewed at 1024 x 768 resolution on Internet Explorer 6.0+ or Mozilla Firefox 1.5+ entry views: 780 today's page views: 911 (23 mobile) all-time page views: 3833264 most viewed entry: 18739 views most commented entry: 14 comments number of entries: 1279 page created Wed Jul 22, 2026 02:59:48 |
|
- tagcloud - academics [70] art [8] changelog [49] current events [36] cute stuff [12] gaming [11] music [8] outings [16] philosophy [10] poetry [4] programming [15] rants [5] reviews [8] sport [37] travel [19] work [3] miscellaneous [75] |
|
- category tags - academics art changelog current events cute stuff gaming miscellaneous music outings philosophy poetry programming rants reviews sport travel work tags in total: 386 |

| ||
|
It's probably time for another check-in on the coronavirus front after mostly laying off the subject since June, and before continuing, I'd like to state that all the following is written in my personal capacity. To start off on a bright note, GEOTUS appears to have given the virus the ol' smackdown - if with a teeny bit of help from Singapore's own National Centre for Infectious Diseases (NCID). The NCID seems to have been doing some good work with convalescent plasma (as advanced here in May), with the antibody cocktail involved in his swift recovery developed from several local patients in collaboration with Regeneron, an American biotech firm. It seems quite likely that some of these donors were foreign workers, given our distribution of cases, which seems to have inspired devoted medical cost-cutter GEOTUS to pay it on; not only has he declared that he wants the same treatment available for free to all his people, he has moreover committed to donating his own plasma, a forthright gesture if ever there was one. Well, one doesn't rise to his position by allowing a glorified flu to get him down, though one suspects that sections of the mainstream press were rooting for martyrdom instead. Ahem, okay, tuning troll mode down... On Test Accuracy - technically, perhaps not entirely unsubstantiated? Everyone's been bombarded by scary headlines for months now - 1,426 new cases here! It's over ninety thousand in India! - that it's often easy to neglect how much uncertainty there can exist, in the testing procedure. A layman might be easily forgiven for believing that the exalted physicians are making an absolute pronouncement, when they declare a patient either COVID-free or COVID-stricken, after administering a test; as it happens, the reality is... not so clean and simple. Let's begin with some basics of medical testing. The sensitivity of a test is defined as the percentage of subjects who are identified as positive for a disease by that test, out of all subjects that actually have that disease. The specificity of a test is defined as the percentage of subjects who are identified as negative for a disease by that test, out of all subjects that actually do not have that disease. From this, a perfect test would have sensitivity and specificity both equal to 1; it always correctly identifies all subjects with the disease, and also always correctly identifies all subjects without the disease. It's probably safe to say that currently-available tests are, almost without exception, not perfect. Beginning with polymerase chain reaction (PCR) swab tests, oft regarded as the gold standard - they're supposedly near-perfect if done correctly... and if the subject has been infected for a week or more, to which perhaps another week might have to be tacked on for the results to be returned. Serological tests, in contrast, can have results known in hours, but despite relatively high (self-?)reported specificities under what one suspects are near-ideal conditions, independent evaluations suggest that for reasonable sensitivities >80%, typical specificities tend to be around 95-99%. Abbott's 15-minute rapid test claims 98.5% specificity, for example, but given that the White House is pushing it hard, The Atlantic for one is having second thoughts, but that's life. Their concern about the specificity does stand, granted. Assume a test specificity of 99%. This implies that for every one hundred healthy persons tested, one will be wrongly identified as having the coronavirus (a "false positive"). Let's say a country tests ten thousand people a day, not too much of a stretch given that many of them are testing some 0.1% of their population daily; even if that country were entirely coronavirus-free, the test specificity would imply that around 100 false positives would be reported. In actuality, test performance can conceivably be rather worse, especially for alternative methods; the CDC admitted that its antibody tests could have a positive predictive value of less than 50%, as is the case in India, with external evaluation suggesting around 80% sensitivity/70% specificity for some test kits - not great, to say the least.  Hitting it between the ears! (Source: straitstimes.com) Given that some countries seem to be reporting new case rates apparently below what typical test specificities would suggest for baseline false positive calls, one has got to suspect that some additional tweaks might have been applied. Among the most obvious is repeat testing (possibly with a different/more accurate test method) to confirm initial positives, which has thrown up its fair share of false positives locally. And this is before one delves into the nitty-gritty of how high the viral load should be, for a person to be considered as afflicted. For PCR, the number of amplification cycles applied seems to be a "hidden parameter" that is seldom expounded on, which has led to much griping about whether some jurisdictions are setting tests to be far too sensitive, and whether subjects identified from such thresholds are actually contagious in practice. Hopefully, the above has begun to inform on how nebulous case statistics for the coronavirus can be, from the scientific angle alone. But what about deaths, one might ask. Surely, it doesn't get more clear-cut than that? If a patient unfortunately passes away, and the body is tested and found to contain the virus, then surely that's a coronavirus death? Well, an exaggerated example might serve to illustrate the difficulty here: consider a motorcyclist who sadly lost an argument with a speeding trailer truck. The paramedics have dutifully scraped his remains off the asphalt and sent them for testing, per procedure, and it turns out that he was positive for COVID-19. Question: did this motorcyclist perish from the coronavirus? Answer: this is a very good question! Generally speaking, there are many possible definitions as to what constitutes death from a disease, and the coronavirus is no expection. For example, as far as is known, Singapore follows the WHO definition in not including non-pneumonia fatalities; in other countries, the criteria can be far more conservative, e.g. Sweden considering everyone dead after testing positive as coronavirus deaths, regardless of how much the virus contributed to the death. Now, neither approach is wrong - it's just that it is clearly unfair to compare death tolls reported under different definitions. Indeed, simply switching definitions (as done by Public Health England) can change the picture quite a bit, though it's probably best to provide more context with finer-grained classifications as to primary, secondary and tertiary deaths, as with the CDC revealing that some 94% of coronavirus deaths had possibly contributing comorbidities. Let's All Be Positive (Or Not)! And now, we venture into the yet-murkier less-scientific considerations. As an instructive example, one might consider a large federal constitutional republic, composed of some fifty states (Country A), and reason as to whether this polity would be biased towards reporting a higher or lower case load and death toll. To begin with, being a good democracy, Country A has passed legislation to pay hospitals a considerable sum of money, for each patient listed as coronavirus-positive (US$13,000, going up to over US$35,000 if they are ventilated) Not to cast aspersions on the integrity of hospital personnel, but it sure seems that this would likely have encouraged them to play it very safe, and with a mostly clean conscience to boot. It never hurts to be cautious, after all? Moving up to higher levels of administration, reporting a higher case and death load would also justify more resources from the Feds (recall the ventilator bidding war between states?), while making the federal government look bad at the same time, which is a nice bonus when they're manned by the opposing party. Note, this is not to assert whether the chosen standards were or were not the most appropriate, given the very-real trade-offs. The point is that the incentives line up towards a liberal interpretation of infection. Next, consider a one-party state (Country C). Here, there are essentially no independent healthcare or media bodies. There's a constant dribble of new cases being reported - usually in the double digits for a population of well over a billion, if they bother to report it at all - despite cities somehow arbitrarily entering lockdown. Even at the height of the pandemic, entire provinces with thousands of already-admitted cases, would claim essentially zero new infections. The head honchos explicitly warned that local officials would be held responsible, were a single new case to be reported. Not to cast undue aspersions on Country C either, but one understands why their purported figures are being left out of official analyses. Oh, it gets more complicated. How many nations are really going to tell each other, Country A or Country C (but especially the latter) that we don't believe you, your numbers are bullshit? Occasionally, one comes across (entirely reasonable) musings about how a place with approximately zero community cases - out of a population of millions - keeps having positive cases detected from the tiny fraction of approved overseas travellers by other countries in reciprocal PCR testing, but the unsaid agreement appears to be not to question the discrepancy, with a wink and a nod. One can only imagine the amount of second-guessing going on as countries seek to establish travel bubbles and fast lanes, as to who's trustworthy, who's not, and who's not but are you gonna be the one to tell them that? Finally, there are the... less-developed states, which might not have been testing that much, because there wasn't all that much money for basic healthcare to begin with (which makes the call to prayer by some health ministers somewhat more relatable); thankfully, many of these states have their population skewing particularly young too, long recognized as a key mitigator aiding survival. It might be considered that some estimates have upwards of a quarter of the populace having already contracted the coronavirus in certain cities, with the WHO's best estimate being 10% of the global population having already gotten it - or about twenty times the "official" case count of about 37.5 million as of today. With statistics like this, who needs facts? Democracy's Due To this mishmash of conflicting standards and perverse incentives, one metric has stood out - excess mortality. The reasoning behind this is fairly simple: it can be exceedingly complicated to tease out the true impact of the coronavirus, given all the heterogeneities between nations, and that's assuming they're being honest with the details. Instead, calculating "how many additional people died this year" requires only accurate annual death figures, and if it is assumed that the coronavirus is the major factor in these extra deaths, a reasonably robust ballpark figure can be arrived at. Looking at this excess mortality data, there is always the danger of being too sweeping with one's pronouncements, but it's sure looking like one of the biggest drivers of coronavirus deaths is... Western democracy. 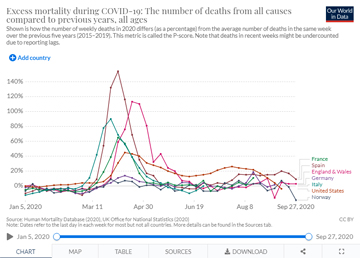 Excess mortality by percent, selected European countries (Source: ourworldindata.org) The genesis of this analysis, as so often happens, is GEOTUS, who made repeated claims in August that Europe had an excess mortality of somewhere between 30% to 40% higher than the United States, in various press briefings. This naturally brought the full weight of the fact-checkers down on him, and it seems like there might have been some hyperbole involved. However, it might be instructive to also note that for all the brickbats slung at America, their performance on coronavirus as compared to comparable Western democracies seems... pretty smack dang average. Perhaps nothing to shout about, but nothing particularly out of the ordinary either. 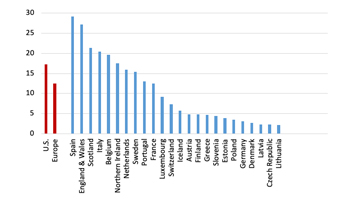 Cumulative P-scores of excess mortality, weeks 9 to 30 (Source: voxeu.org) Two Oxford researchers have supplied a fairly comprehensive analysis on comparative excess mortality, which does appear to suggest that some European nations have been worse off than the U.S., namely Spain, Italy, Belgium, and the United Kingdom. France, Sweden, Portugal and the Netherlands aren't too far off either, and the major Western European outlier would seem to be Germany. From Table 3 in the report, the cumulative P-score for the peak eleven weeks seems largely comparable for all major European countries and the U.S., and for raw excess deaths per million, America indeed also comes solidly in the middle of the pack at 627/M, compared to say Spain's 1057/M or France's 448/M. Moreover, excess deaths appear highly unbalanced regionally for the U.S., with the northeastern region (including New York) recording 1473/M, which I believe would imply an excess death rate of around 454/M for the rest of the U.S. - which would put them near the bottom of the table. Again, this is not to downplay the pandemic, or to expressedly laud/denigrate the response of any of the countries studied (although it could be noted that the press frenzy and hysteria has applied to some of them far more than others in comparable situations). The point, instead, is more towards asking: what more, realistically, could have been done? With the benefit of hindsight, one might certainly provide answers with some confidence - ban foreign travel, especially from countries known to have an outbreak; then, institute a heavy lockdown with widespread testing and quarantine, and be prepared to block travel between local regions if required; also, mandate universal masking. Few if any countries have managed to strike the jackpot on this - perhaps New Zealand? - and it might be remembered as to how prevailing best scientific advice was wholly against international travel bans (additionally decried as racist and xenophobic, mind) and face masks, until it didn't matter quite as much any longer. The main takeaway, I'd say, would be that guaranteed personal liberties do come with a price - that of possibly making suboptimal decisions for the wider society. Yes, if one were given free reign to minimize deaths from the pandemic as the overriding objective, the reponse would probably be a lot closer to China's - draconian travel restrictions with residents confined to their homes, sentencing and heavy fines for the slightest flouting of regulations, for whatever reasons. Trouble is, they have individual rights in America and Europe, rights for which many lived for, bled for, died for; take for something as seemingly commonsensical as a hard lockdown on the New York/New Jersey/Connecticut tri-state region, when the coronavirus was running entirely wild there in March; you had the Governor arguing that it was illegal, and indeed, it was probably to the benefit of the residents of the region to be able to leave if they wanted. Of course, what's good for the relatively few might not be also good for the many, but it was their right. Was there any getting around this foundation of Western democracy? From the empirical evidence, I suspect not. [To be continued...] Next: Corona Update (Part II)
|
|||||||
 Copyright © 2006-2026 GLYS. All Rights Reserved. |
|||||||




